
Superior Mesenteric Artery Syndrome: A Hypermobile Dietitian's Guide
We’ve seen an increasing number of diagnoses of abdominal vascular compression syndromes like Median Arcuate Ligament Syndrome (MALS) and Superior Mesenteric Artery Syndrome (SMAS) in our clients over the past few years, thanks to the ongoing efforts of medical practitioners and patient advocates raising awareness in the Hypermobility space.
Surprisingly (at least to me), I was diagnosed with SMAS in late 2024. Looking back over my lifetime of digestive concerns and other health quirks that were often put down to anxiety, in retrospect this makes a great deal of sense and has provided a HUGE feeling of validation.
Here is my overview about SMAS in Hypermobility conditions.
What is Superior Mesenteric Artery Syndrome?
@hypermobility.dietitian
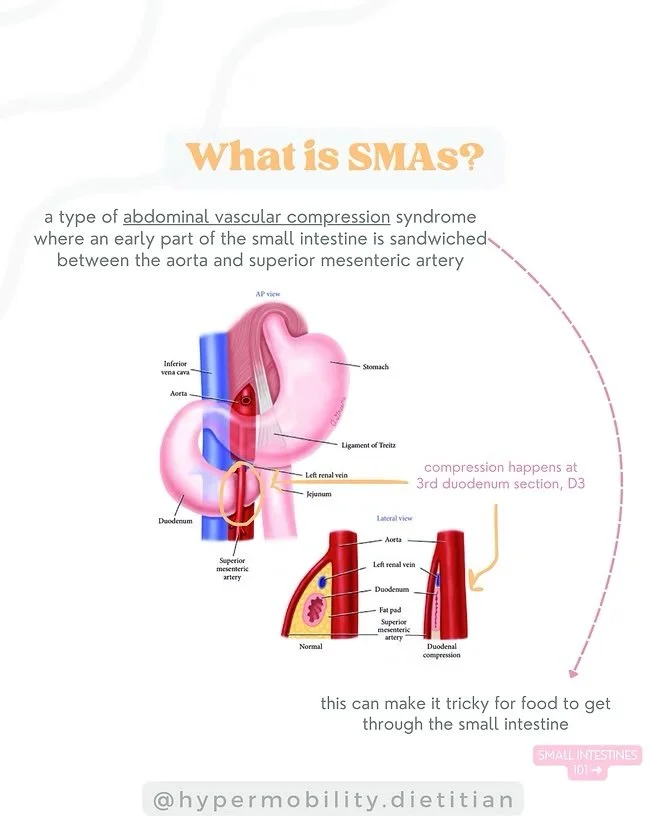
Abdominal vascular compression syndromes (AVCS) occur when something is either squishing or being squished by a blood vessel, in the abdominal cavity.
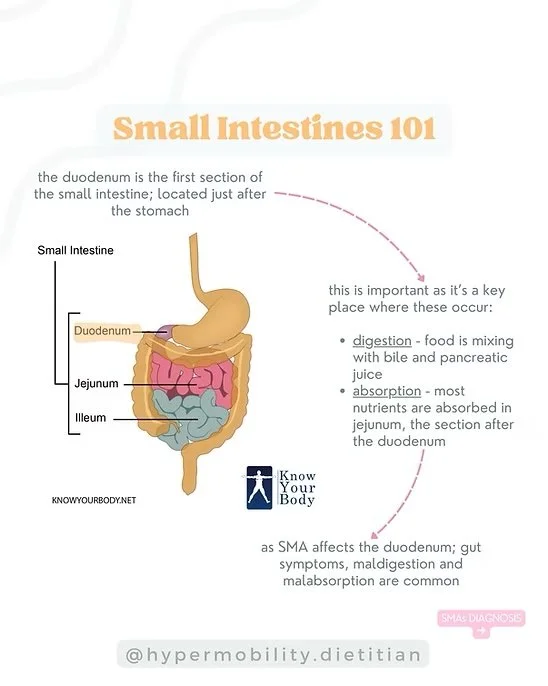
In SMAS, an early part of the small intestine is sandwiched between the superior mesenteric artery and aorta, making it difficult for food to get through. Specifically, compression occurs at the 3rd part of the duodenum (D3). The duodenum is the first section of the small intestine located just after the stomach.
The structure of our small intestines are as follows:
Duodenum - a short, 10 inch section with four sub-sections. D1 receives receives partially digested food from the stomach. D2 is where bile & pancreatic juice are delivered to facilitate protein & fat digestion (and more!). D3 is a horizontal section which runs between the aorta and superior mesenteric artery and D4 delivers partially digested food into the jejunum.
Jejunum - moderately long section of the small intestine which works to further digest and absorb nutrients. Large folds in the lining of the jejunum, and finger-like projections called villi increase surface area to maximise absorption.
Ileum - the longest section (~3.5m) of the small intestines which further absorbs nutrients, and can also absorb water.
@hypermobility.dietitian
Why can SMAS develop in Hypermobility conditions (e.g. HSD, hEDS)?
Science is still not fully sure why SMAS develops in people with hypermobility conditions. A few of the current theories are:
Reduced duodenal fat pad - usually there is a protective fat pad cushioning the D3 section of the duodenum from surrounding arteries. If a period of significant (and/or rapid) weight loss or malnutrition has occurred at any point, this increases the chance of this fat pad wasting.
Altered anatomy due to hypermobility, such as visceroptosis. Visceroptosis happens when organs 'droop' lower than they're meant to in our abdominal cavity, due to altered connective tissue from HSD/hEDS and potentially from muscle wasting due to malnutrition. Severity of visceroptosis and which organs are impacted can vary significantly, but ultimately if organs aren't sitting where they are meant to, the risk of vascular compressions at certain points increases significantly.
Potential connective tissue remodelling due to hEDS or HSD. This is an emerging area, and something that we are still learning more about.
How is SMAS diagnosed?
SMAS can be diagnosed by various procedures and tests, by several key medical specialties.
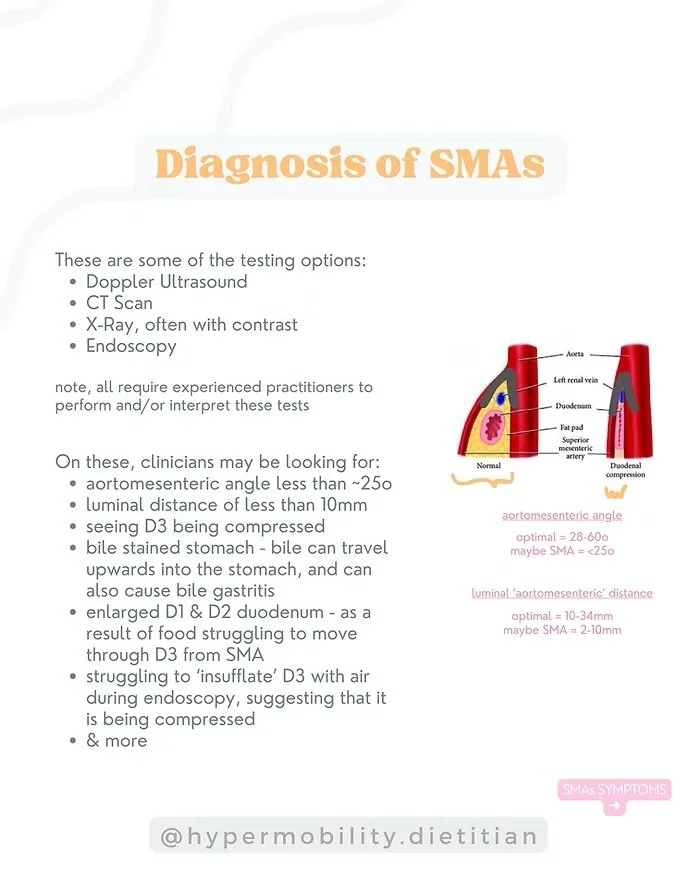
Some of the testing options include:
Doppler Ultrasound (this is the most readily available in Australia)
Often people have other intra-abdominal vascular compressions checked at the same time, such as Median Arcuate Ligament Syndrome, May-Thurner Syndrome and Nutcracker Syndrome
CT Scan
Endoscopy (see this journal article for in depth discussion of features to observe - and photos!)
X-Ray with contrast
Note: all of the above generally require experienced practitioners to perform and/or interpret these tests. We have seen many cases of SMAS being initially dismissed until a more knowledgeable practitioner reviewed the results, redid the test themselves, or ordered the test at a facility which uses more advanced protocols.
Often people have other intra-abdominal vascular compressions checked at the same time, such as Median Arcuate Ligament Syndrome, May-Thurner Syndrome and Nutcracker Syndrome.
On these, clinicians may be looking for:
Aortomesenteric angle less than ~25 degrees
Duodenal luminal distance of less than 10mm
Seeing D3 section of the small intestine being compressed or narrowed
Bile stained stomach or oesophagus, due to bile travelling upwards from SMAS. We often see gastritis as a result of this and other causes in SMAS.
Large volume of liquid in the stomach despite fasting, and or gastroptosis (drooping of the stomach, making it difficult for contents to exit).
Enlarged D1 & D2 duodenum, as a result of food struggling to move through D3 from SMAS
Struggling to 'insufflate' D3 with air during endoscopy, suggesting it is being compressed
During endoscopy, air is blown into the intestines to allow the clinician to see what's going on (and take the pretty pictures we've all seen on google images and medical textbooks) - this is called 'insufflation'
Reverse peristalsis at D1 & D2, due to food struggling to pass D3
And more
Symptoms of SMAS
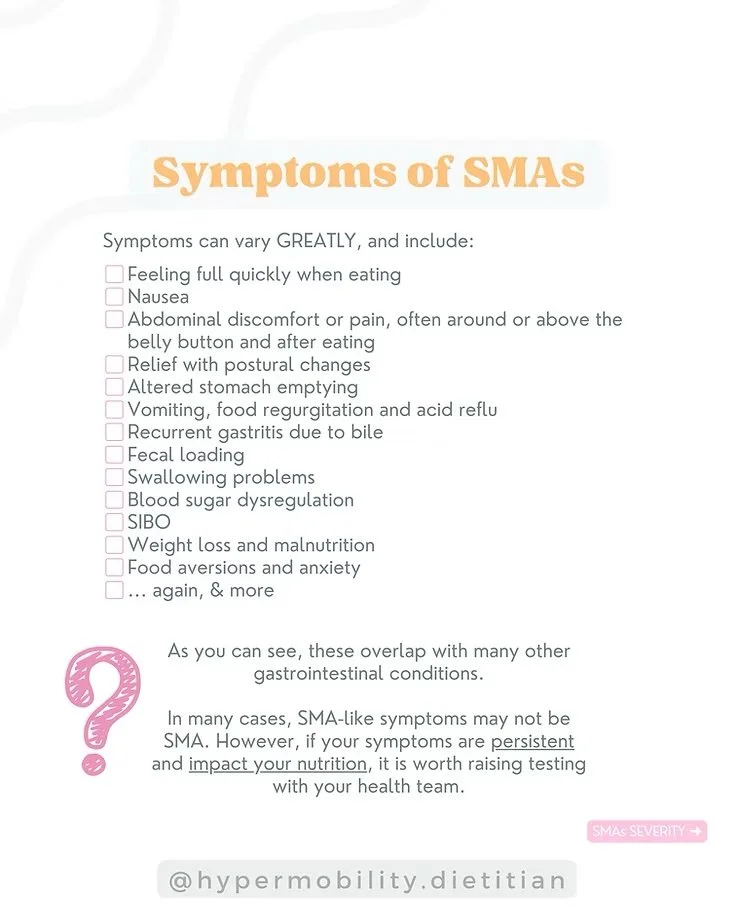
Symptoms can vary GREATLY, and include:
Feeling full quickly when eating
Nausea, often starting 15-30min after eating
Abdominal discomfort or pain, often around or above the belly button after eating
Altered stomach emptying
Vomiting, food regurgitation, acid/bile reflux and difficulty swallowing
Recurrent gastritis
Weight loss, anxiety around food and malnutrition
Relief with lying in a prone position (on belly) or in left lateral decompression (fetal position on left hand side)
Reactive hypoglycaemia and other blood sugar regulation problems
Malabsorption of protein and fat (fatty, sticky, smelly and sometimes pale stools)
We often see SMAS co-exist with other conditions, including:
Connective tissue disorders like hypermobile Ehlers Danlos Syndrome (hEDS) and Hypermobility Spectrum Disorder (HSD)
Postural Orthostatic Tachycardia Syndrome (POTS) and other dysautonomias
Mast Cell Activation Syndrome (MCAS)
Small Intestine Bacterial Overgrowth (SIBO) - likely due to impacted gut motility and food transit making favourable environments for opportunistic bacteria to overgrow
Visceroptosis and Gastroptosis
Gastroparesis (slow stomach emptying) and dumping syndrome (rapid stomach emptying)
Pre-diabetes, insulin resistance, PCOS
Disordered eating and eating disorders (including Anorexia Nervosa, ARFID, Bulimia)
Malnutrition
Left renal vein compression (Nutcracker syndrome), as this often runs parallel to the duodenum and is also compressed by the SMA at D3
NOTE: As you can see, these symptoms overlap with many other gastrointestinal conditions. In many cases, SMAS-like symptoms may not be SMAS.
However, if your symptoms are persistent and impact your nutrition, it is worth raising testing with your healthcare team.
How severe is SMAS?
While an SMAS diagnosis can feel daunting, its severity varies widely. Until recently, most diagnoses have been in people with severe symptoms. However, at recent medical conferences, clinicians have shared that SMAS may be more common than we realise - especially in people with hypermobility conditions, and that many individuals might actually be asymptomatic
Most of my SMAS clients can manage their nutritional intake and symptoms via diet quite well, only requiring conservative management (e.g. POTS & MCAS medication, mild dietary strategies) - and they live full lives with relative ease.
Some people with SMAS may need more intensive treatment, such as enteral feeding. This can involve using a nasojejunal tube, which is inserted through the nose and delivers nutrition directly past the SMAS compression into the small intestine. Nasogastric tubes, which feed into the stomach, are not recommended because they don’t bypass the compression. For longer-term feeding, a surgical tube may be inserted through an stoma into the small intestine (a PEJ or J-tube). Some patients may have a G-J tube, where the stoma enters the stomach but the feeding tube is connected to the small intestine, bypassing the compression. In some cases, patients who require ongoing enteral nutrition also benefit from a tube in the stomach to remove excess fluid and bile, and to administer medication.
For clients who are severely impacted, 'parenteral nutrition' is sometimes considered. This feeds completely broken down nutrition directly into the vascular system.
See our blog post on ‘Understanding Tube Feeding Pathways for EDS and Hypermobility in Australia’ for more information about enteral and parenteral nutrition.
SMAS Dietetic Management
Given the range in severity with SMAS symptoms, exact nutrition strategies can vary person-to-person. There are a few common themes:
Keep up food intake and avoid further malnutrition | rapid weight loss, whether from low food intake or absorption can waste the fat pad around D3 and result in muscle loss, potentially worsening symptoms. If you notice signs of malnutrition increasing (see here for how Dietitians assess malnutrition in Australia - noting that an overall 'A' score means at risk of malnutrition, 'B' means moderate malnutrition and 'C' means severe malnutrition), chat to your healthcare team.
Postural changes | play around with how you position your body when eating, digesting and generally sitting. Left lateral decompression (lying in fetal position on LHS), and lying flat on your belly in a prone position (or supported with cushions in a child's pose like position) are worth trying and often help. The Hayes manoeuver (applying gentle pressure bellow the bely button, directed upwards towards the chest and slightly towards the back) is often reported in published case studies to temporarily reduce duodenal compression. Work with your physiotherapist to identify if you have lumbar lordosis (excess lower back curve), and if yes, work on reducing this as it can compress D3 further.
Clear fecal loading | this is very common in hypermobile humans, and can significantly impact overall gut motility, inflammation (via mast cells and nervous system), microbiome and more.
Keep on top of dysautonomia and MCAS | this will support better autonomic nervous system function and inflammatory responses, which have many relevant impacts including reducing visceral hypersensitivity (organ pain).
Make a malnutrition action plan | chat to key people in your health team - what steps are within reach to reduce malnutrition from worsening (if present) or occurring? When is it time to seek additional help, and where can you go? How can you adapt nutrition during these times? Noting that waitlists often take several months-years.
In summary, I hope this has brought a bit more clarity around what SMAS is, and life with abdominal vascular compressions. If you are currently diagnosed with SMAS or looking into diagnosis, I'm sending you gentle virtual hugs - I know the journey can sometimes feel long, but with the right support and strategies, finding ease and clarity is absolutely possible.
Savvy
Disclaimer: the information above is for education purposes only.
This blog post was published on 7th January 2025, and received 2,290 views before migrating website platforms in January 2025.